Click on the links below to find out more






SCFE- Slipped Capital Femoral Epiphysis
Treatment
The goal of treatment is to prevent the displaced femoral head from slipping any further. This is accomplished by surgical stabilisation of the hip. Early diagnosis gives the best chance of stabilizing the hip and avoiding complications. When treated early and appropriately, long-term hip function can be expected to be very good. Once SCFE is confirmed, your child will not be allowed to bear weight on his or her hip and will be admitted to the hospital for surgery.
Procedures
The surgical procedure Mr Slattery recommends will depend upon the severity of the slip. Procedures used to treat SCFE include:
- In situ fixation: for stable or mild SCFE. Mr Slattery makes a 1-2cm incision over the hip and inserts a metal screw to hold the hip in place to prevent further slippage.
- Hip Arthroscopy: this is keyhole surgery which can be done at the same time as in situ fixation to reshape the femur to prevent femoroacetabular impingement (FAI) occurring.
More information about Hip Arthroscopy here - Capital Realignment: this is a highly specialized procedure that involves cutting the femur bone to safely dislocate the hip and reposition the ball of the hip on top of the thighbone to restore the alignment and anatomy of the hip. This is generally only done for the most severe slips which are at high risk of developing complications
- Opposite Hip Fixation: Some patients are at high risk for SCFE occurring on the opposite side, if this is the case Dr Slattery may recommend inserting a screw the unaffected hip at the same time to reduce the risk of SCFE.
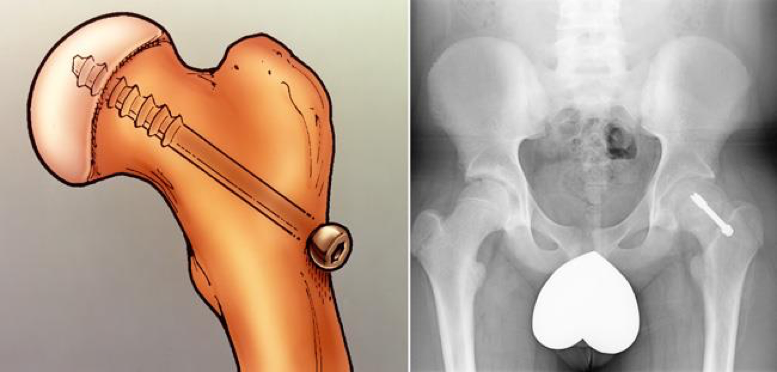
Illustration and x-ray of in situ fixation. A single screw has been inserted to prevent the slip from getting worse.

In this x-ray, two screws have been inserted in the patient’s right hip to stop progression of a slip. A single screw has been inserted in the left hip to prevent SCFE from developing.
Complications
Although early detection and proper treatment of SCFE will help decrease the chance of complications, some patients will still experience problems.
The most common complications following SCFE are femoroacetabular impingement (FAI), avascular necrosis and chondrolysis.
Avascular Necrosis
If severe cases, SCFE causes the blood supply to the femoral head to become limited. This can lead to a gradual and very painful collapse of the bone—a condition called avascular necrosis (AVN) or osteonecrosis.
When the bone collapses, the articular cartilage covering the bone also collapses. Without this smooth cartilage, bone rubs against bone, leading to painful arthritis in the joint. For some patients with AVN, further surgery may be needed to reconstruct the hip.
AVN is more likely to occur in patients with unstable SCFE. Because evidence of AVN may not be seen on x-ray for up to 12 months following surgery, the patient will be monitored with x-rays during this period of time.
Chondrolysis
Chondrolysis is a rare but serious complication of SCFE. In chondrolysis, the articular cartilage on the surface of the hip joint degenerates very rapidly, leading to pain, deformity, and permanent loss of motion in the affected hip.
Although the cause of the condition is not yet fully understood, it is believed that it may result from inflammation in the hip joint.
FAI (Femoroacetabular impingement)
When the head of the femur slips, and is fixed without being put back into its natural position it distorts the normal ball and socket relationship of the hip joint and this commonly results in femoroacetabular impingement (FAI). This can lead to loss of motion within the hip joint, difficulties with sports, and is a leading cause of arthritis later in life. For more information about FAI, click here.
Recovery
Weight Bearing
After surgery, your child will be on crutches for several weeks. Dr Slattery will give you specific instructions about when full weight bearing can begin. To prevent further injury, it is important to closely follow these instructions.
Sports and Other Activities
For a period of time after surgery, your child will be restricted from participating in vigorous sports and activities. This will help minimize the chance of complications and enable healing to take place.
Follow Up
Your child will return for follow-up visits after surgery. These visits may include x-rays every 3 to 4 months to ensure that the growth plate has closed and that no complications have developed.
Depending upon the patient’s age and other factors, a team approach that includes a general paediatrician, endocrinologist, and/or dietician may be necessary for comprehensive care in the long run.

Dr David Slattery
FRACS MBBS (Hons) LLB FAOrthA
Dr David Slattery is an orthopaedic surgeon based in Melbourne with over 10 years of experience, with a special focus on hip and knee joint preservation and replacement. With qualifications in both medicine and law, he brings a unique and comprehensive approach to patient care. His surgical techniques are minimally invasive and evidence-based, designed to reduce pain and enhance recovery.
Trained in leading institutions across Europe and the USA, Dr Slattery offers advanced treatments for a wide range of joint conditions. He is deeply committed to patient outcomes and takes pride in tailoring treatment plans to each individual. Whether you’re an athlete or seeking relief from chronic joint pain, his goal is to restore function and improve your quality of life.
To book an appointment please contact Dr Slattery’s rooms on
03 9819 6934

We aim to see all fractures within 24hrs